A 21yr old male with Diabetic ketoacidosis with denovo detected DM with viral pyrexia
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.



















 HbA1c:
HbA1c:
 PLBS:
PLBS:


Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.”
A 21year old male resident of miryalaguda came to casualty with chief complaints of
fever since 5 days, c/o decreased appetite since 7days, c/o vomiting since 1day, c/o sob since morning.
Patient was apparently asymptomatic 5days back then he developed fever which was insidious in onset, intermittent and was of high grade type a/w chills and relieved on medication. Pt had h/o 1episode of vomiting 1day back which was non-bilious,non- projectile.
No h/o any burning micturition, throat pain, cold,cough.
PAST HISTORY:
Not a k/c/o HTN,DM, CAD, asthma, TB, epilepsy.
PERSONAL HISTORY:
Patient has mixed diet with normal appetite and adequate sleep.
he has normal bowel movements and bladder filling.
No addictions.
No significant family history or allergic history.
GENERAL EXAMNATION:
Patient is c/c/c ,moderately built and moderately nourished.
No pallor, icterus, cyanosis, clubbing, lymphadenopathy, pedal edema.
VITALS:
BP: 140/90 MMHG,
PR: 120bpm
Temp: 98.2°F,
RR: 40 CPM,
SPO2: 99%
RS: BAE+,NVBS heard
CVS: S1 ans S2 heard. No murmurs.No thrills
P/A: soft and non-tender.
CNS: No focal deformities.
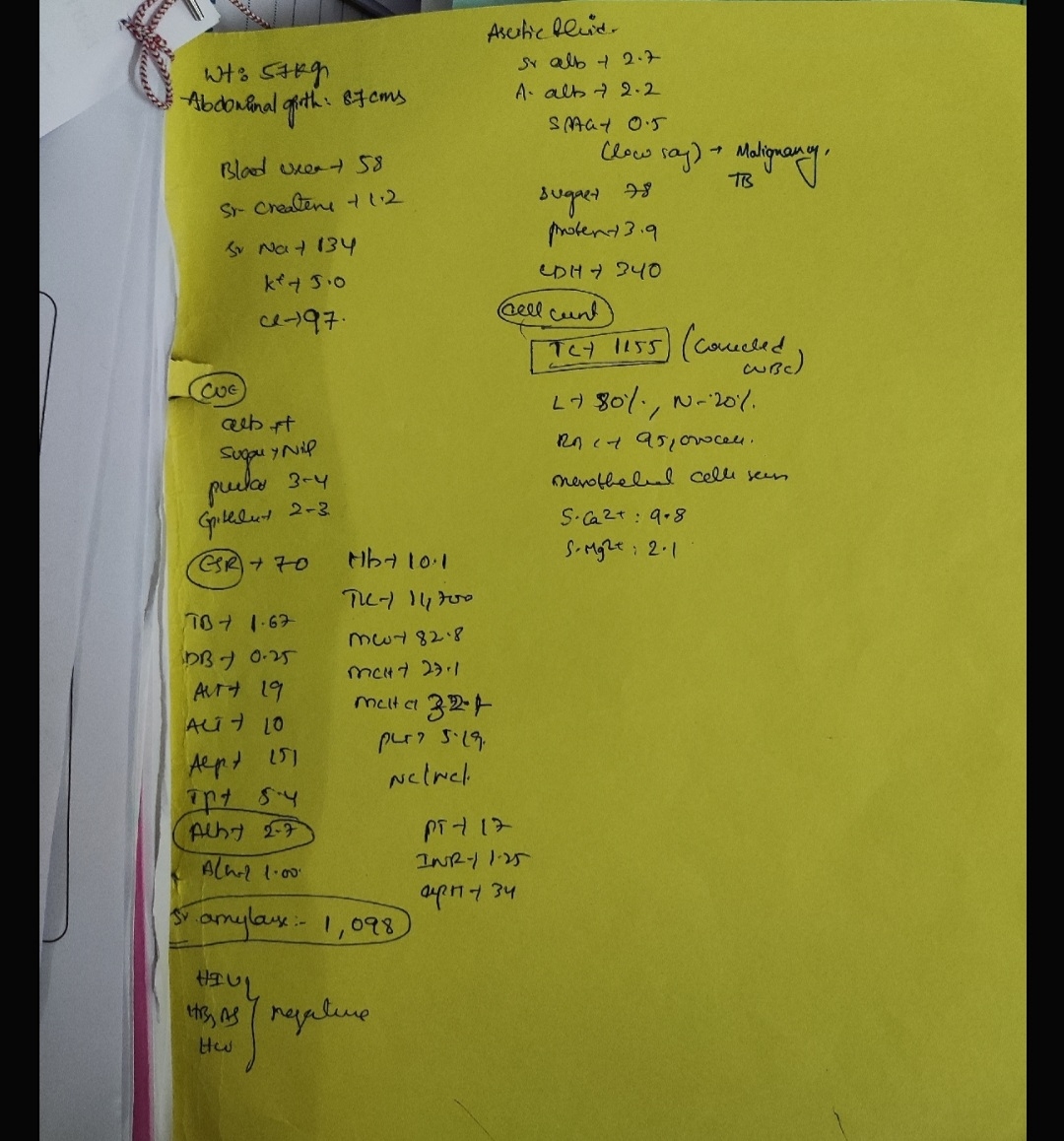
INVESTIGATIONS:
1) HEMOGRAM :
Hb: 8.2
TLC: 15800
N:89
L:6
PCV: 30
Mcv:63.7
MCH:17.4
MCHC:27.3
PLC:3.37
RBC:4.71
2) LFT:
3)CUE
4)RBS:194
5)BLOOD UREA:29
6)SERUM CREATININE:0.8
7)URINE FOR KETONE BODIES:
8)ABG@2PM
9)SERUM ELECTROLYTES @2pm

S.ELECTROLYTES@ 10PM
10) Chest xray PA view:
PROVISIONAL DIAGNOSIS:DIABETIC KETOACIDOSIS WITH DENOVO DETECTED DIABETES MELLITUS WITH VIRAL PYREXIA UNDER EVALUATION
TREATMENT:
On DAY-1
1)NBM till further orders
2)IVF 3lit NS @500ml/hr(in 3hrs) f/by IVF NS@250ml/hr
3)Inj. HAI 4IU IV/stat f/b Inj. HAI 1ml (40IU) in 49ml NS @ 4ml/hr(untill ABG correction)
4)Inj. PAN 40mg IV/OD
5)IVF 5%DEXTROSE @50-100ml/hr(when GRBS <150) [increase/decrease acc. to GRBS]
6)Inj.OPTINEURON 1amp in 100ml NS/IV/OD
7)GRBS monitoring hourly
8) Strict i/o. Monitoring
9)Inj. KCl 2amp in 500ml NS @100ml/hr
On DAY-2 :
SOAP NOTES:
S:
No fever spikes,sob decreased ,no fresh complaints
O:
BP-110/90mm hg
PR-74bpm
CVS:S1S2 heard
Rs:BAE +,NVBS
P/A:soft
A:
HAGMA, DKA
Hemogram:
ABG @1AM
@8AM
@3PM
S.ELECTROLYTES:@8AM
@5PM
@10.30PM
P:
1)IVF 0.45% NaCl,RL @100ml/hr
2)Inj. KCl 2amp in 500ml NS @100ml/hr
3)Inj. HAI 1ml (40IU) in 39ml NS @ 4ml/hr(untill correction of acidosis)
4)Inj. PAN 40mg IV/OD
5)Inj.OPTINEURON 1amp in 100ml NS/IV/OD
6)GRBS monitoring hourly
7)Strict i/o. Monitoring
8)NBM till further orders
DAY-3 :
S: Patient sob decreased,No fresh complaints
O: BP 110/80 mm hg
PR: 70 bpm
CVS: s1 s2 heard
RS: BAE+ NVBS
P/A: soft
ABG@6.30AM
S.ELECTROLYTES @8AM
Assesmemt : over night patient grbs around 290 mg/dl and Patient anion gap is reducing day by day and subjectively feeling better .
Plan of care : Look for today morning abg and stop iv insulin infusion and start him on NPH and HAI
DAY-4
Pt shifted to AMC
S: no fresh complaints
O: BP130/80 mm hg
PR 80 bpm
CVS: s1 s2 heard
RS:BAE + NVBS
P/A: soft,non tender
Assesmemt :
DKA
GRBS 157mg/dl
FBS :114 mg/dl
Hemogram:
Plan :
Stopped insulin infusion
Started Inj. NPH S/C according to grbs(8am---2pm---8pm)
Inj.HAI S/C acc to grbs
IVF NS,RL @100ml/hr
INJ.PAN 40mg
DAY-5
Pt shifted to ward
S: no fresh complaints
O: BP :110/80 mm hg
PR :102 bpm
CVS :s1 s2 heard
RS: BAE+,NVBS
P/A: soft
Assesmemt :
DKA
GRBS 148mg/dl
FBS:111 mg/dl
Plan :
Started Inj. NPH S/C according to grbs(8am---2pm---8pm)
Inj.HAI S/C acc to grbs
Oral fluids
INJ.PAN 40mg
Thrombophobe ointment (l/a over left forearm)

Comments
Post a Comment